Jessica Livermont, BA, Brooke Pankhurst, BSc, and Nathan Lighthizer, OD, FAAO
SIGNIFICANCE: Primary open angle glaucoma is often treated with SLT. Energy from the laser has the potential to adversely affect the corneal endothelium.
PURPOSE: We want to know if the new SLT laser is more protective of the endothelial cell count versus other brands of SLT lasers.
METHODS: We analyzed endothelial cell counts pre and post-SLT with different brands of lasers.
RESULTS: The new SLT laser shows no statistically significant difference in endothelial count before and after the SLT procedure (P = 0.5). The other brand of SLT laser does show a statistically significant loss of endothelial count after the SLT procedure (P = 0.01).
CONCLUSIONS: We want to know if the new SLT laser is more protective of the endothelial cell count versus other brands of SLT lasers.
The thinnest layer of the cornea, the endothelium, is responsible for providing nutrients from the aqueous to the cornea. Endothelial cells can be five or seven-sided, however, the vast majority of cells are hexagonal in shape.1 This arrangement, also called the endothelial mosaic, is preferred due to the area coverage without any gaps.1,2 If any endothelial cell is injured, the cells will not divide and replicate, rather they will migrate and spread to cover the defect.1,3 A normal healthy endothelial cell density in children ranges from 3,000 to 4,000 cells/mm2.1 Cell density decreases gradually with age resulting in a normal cell density from 1,000 to 2,000 cells/mm2 at 80 years old.1 In order for adequate functioning, the cell density cannot be below 400 to 700 cells/mm2 , otherwise loss of transparency and swelling will occur.1,3,4
There has been increasing evidence that glaucoma can cause a loss of corneal endothelial cells.5 Specific types of glaucoma such as primary open-angle glaucoma, primary angle-closure glaucoma, and secondary types of glaucoma have been shown to cause endothelial cell loss, possibly from the compressive mechanism of high intraocular pressure or from cell toxicity due to long-term hypotensive treatments.5,6 The preservative benzalkonium chloride used in topical glaucoma medications is known to cause ocular surface damage and is currently being researched for possible endothelial cell damage.5,6 Glaucoma patients are often on more than one glaucoma drop which can increase the toxicity to the endothelial cells.7 Preservative free glaucoma drops are an option, however, procedures such as selective laser trabeculoplasty also provide IOP lowering effects without the need for patient compliance.8
Selective laser trabeculoplasty (SLT) was first FDA approved in the United States in 2001.9,10 It is a procedure that selectively targets the pigmented cells of the trabecular meshwork.9,11 SLT is a means of lowering internal ocular pressure by increasing aqueous outflow through the trabecular meshwork.9,12 It is a treatment option for primary open-angle glaucoma and ocular hypertension that doesn’t require any patient compliance.13,14 For this reason, it is increasing in popularity as a first-line treatment for glaucoma patients.13-15 The SLT procedure is not a permanent fix, but it can be repeated if necessary.13,15,16 A study published in 2020 by Khawaja et al found that 70% of patients responded to their first SLT procedure.9 They also reported that increasing outflow through the trabecular meshwork can only lower the IOP so much. It is limited by resistance from Schlemm’s canal, collector channels, and episcleral venous pressure.9 The average IOP reduction is anywhere from 16-40% depending on the baseline IOP.8,14,17,18
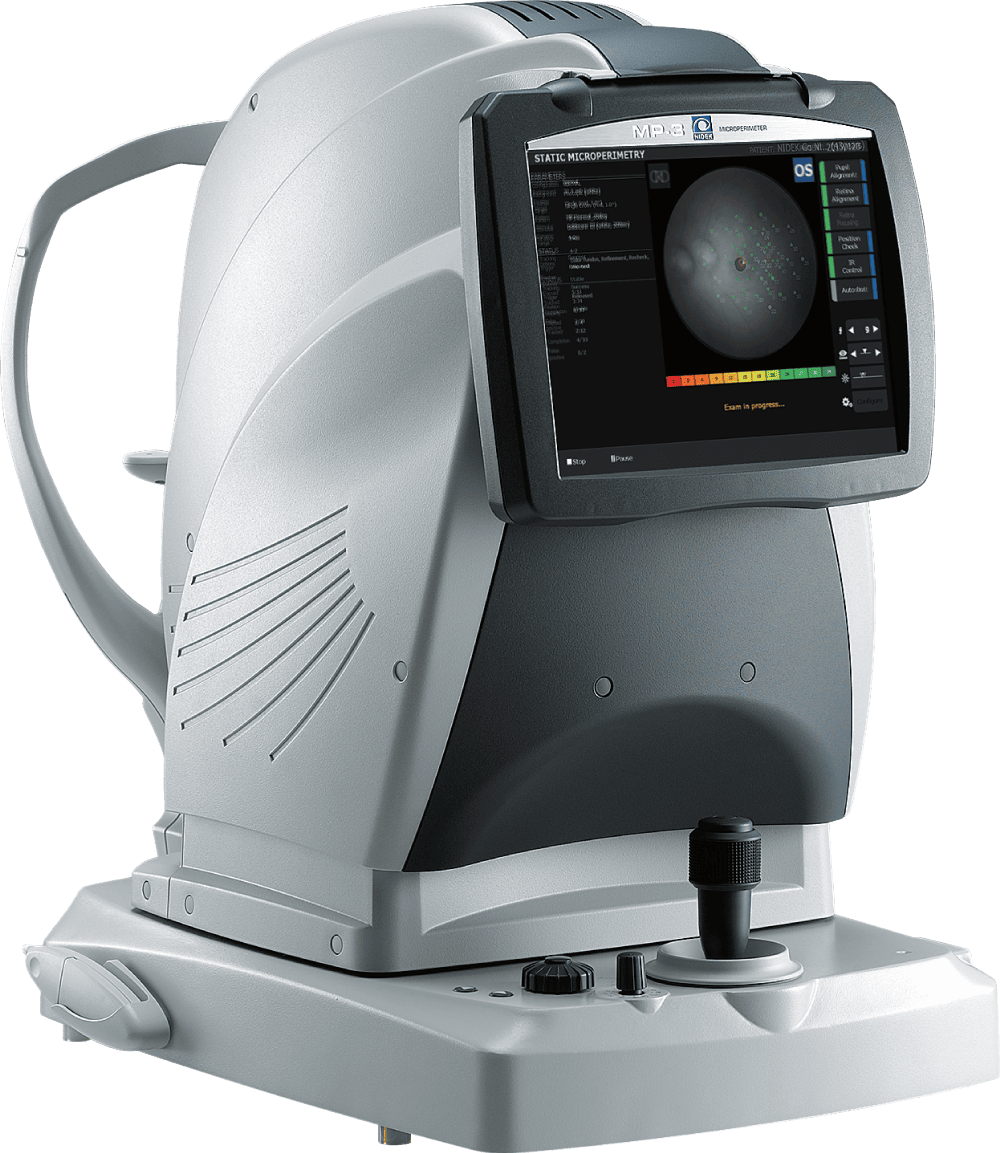
Specular microscopy is used in order to properly assess corneal morphology and structure.19 Noncontact and contact specular microscopy can be used to measure the endothelial cell density (ECD) as well as visualize any morphological changes to the endothelium.4,20 Dark spots are often seen in the endothelium of a normal healthy cornea and can be caused from edema, inflammation, endothelial cell dropout, or inflammatory deposits.21,22 Performing specular microscopy before and after procedures, such as selective laser trabeculoplasty (SLT), provides relevant data about the health of the patient’s endothelium and whether or not they could under designed to better preserve corneal endothelial cells with a newly designed cone angle of the laser at 5.5 degrees which decreases the energy density on the cornea. Other SLT lasers on the market have a cone angle of 3 degrees. This small increase in cone angle lowers the risk of corneal endothelial damage during the procedure. The new SLT company has determined that the threshold limit of safe energy density on endothelial cells is approximately 0.170 J/cm2. They found that an SLT designed with a cone angle of 3 degrees exceeds this safety threshold even at 0.6mJ. The new SLT stays below the safety threshold until approximately 1.4mJ. When performing an SLT the initial power setting is usually between 0.6 – 0.9mJ and can be increased as needed.14
The aim of this study is to compare corneal endothelial cell loss post-new SLT with corneal endothelial cell loss post-new SLT with corneal endothelial cell loss post-other SLT brands. This study is important because patients with an abnormally low endothelial cell count may be at higher risk of adverse effects after an SLT procedure.23,24 SLT is thought to be advantageous over pressure-lowering eye drops in the treatment of glaucoma as it may reduce the lifetime cost of glaucoma treatment for the patient.9 There are no compliance issues with SLT and it is thought to have fewer side effects than pressure-lowering drops.9,25 Endothelial cell preservation would make the new SLT laser system favorable over other SLT brands.
METHODS
This retrospective chart review was supervised by Cherokee Nation Institutional Review Board and co-supervised by Northeastern State University Institutional Review Board. Patient’s informed consent was obtained before data collection. This study included all patients who were undergoing an SLT for the first time to treat ocular hypertension. The only patients excluded from this study were those who had an SLT performed previously. If a patient required an SLT in both eyes, the new laser was used in one eye and a different brand of laser in the other eye to allow for direct comparison. Too remain consistent, the same non-new laser was used. All SLT procedures were performed by licensed optometrists. 1 drop of brimonidine and 1 drop of proparacaine were instilled into the eye prior to the procedure. 1 drop of Alphagan was instilled into the eye after the procedure. Acular was prescribed for post-op discomfort and patients were instructed to use it no more than 4 times a day. Endothelial cell counts were measured before SLT, immediately after SLT, 1 week post-SLT, and 6 weeks post-SLT. The CEM-530 specular microscope was used to measure the endothelial cell counts at each visit.
RESULTS



A paired, two-tail t-test indicates a statistically significant difference in the change of endothelial cell count post-SLT when calculating the overall data (P < 0.05). A separate two-tail t-test was calculated to demonstrate the difference between pre-SLT and 6 weeks post-SLT for each individual laser and its respective data. From this calculation, the new SLT illustrates no statistically significant difference of endothelial count before and after the SLT procedure (P = 0.5). The other brand of SLT laser does indicate a statistically significant loss of endothelial count when comparing pre-SLT and 6 weeks after the SLT procedure (P = 0.01).
CONCLUSION
The purpose of this study was to investigate if the new SLT laser is more protective of the endothelial cell count versus a different brand of SLT laser on the market. We have kept the name and brand of the other laser used in this study confidential. Our statistical analysis indicates that the new SLT did not significantly decrease the endothelial cell count after an SLT procedure. The endothelial counts actually measured slightly higher post-SLT. This increase is likely due to random variations in measurements and is not a genuine increase in cell count. The other laser used in this study was found to have a statistically significant decrease in endothelial cell count after an SLT procedure. However, we do not think this decrease in clinically significant. Further studies should be conducted with larger sample sizes.
REFERENCES
- Remington LA. Cornea and sclera. In: Falk K. Clinical Anatomy and Physiology of the Visual System, 3rd. St. Louis: Elsevier; 2012:10-35.
- Brooks A, Grant GB, Gillies WE. The Identification of Corneal Guttae. Cornea 1991;10:249-60.
- Borkar DS, Veldman PV, Colby KA. Treatment of Fuchs Endothelial Dystrophy by Descemet Stripping Without Endothelial Keratoplasty. Cornea. 2016;35:1267-73.
- Szalai E, Nemeth G, Berta A, Modis L. Evaluation of the Corneal Endothelium Using Noncontact and Contact Specular Microscopy. Cornea 2020;39:567-70.
- Gagnon MM, Boisjoly HM, Brunette I, et al. Corneal Endothelial Cell Density in Glaucoma. Cornea 1997;16:314-8.
- Yu ZY, Wu L, Qu B. Changes in Corneal Endothelial Cell Density in Patients with Primary Open-angle Glaucoma. J Glaucoma 2015;2:286-9.
- Jacobs DS. Open-angle Glaucoma: Epidemiology, Clinical Presentation, and Diagnosis. In: Post T, ed. UpToDate [online]. Available at: https://www.uptodate.com/contents/open-angle-glaucoma-epidemiology-clinical-presentation-and-diagnosis. Accessed June 25, 2020.
- Schultz NM, Wong WB, Coleman AL, et al. Predictors, Resource Utilization, and Short-term Costs of Laser Trabeculoplasty Versus Medication Management in Open-Angle Glaucoma. Am J Ophthalmol 2016;168:78-85.
- Gazzard G, Konstantakopoulou E, Garway-Heath D, et al. Selective Laser Trabeculoplasty Versus Eye Drops for First-line Treatment of Ocular Hypertension and Glaucoma (LiGHT): a Multicentre Randomised Controlled Trial. Lancet 2019;393:1505-16.
- Wood SD, Elam A, Moroi S. Rare Corneal Complication Following Selective Laser Trabeculoplasty. Am J Ophthalmol Case Rep 2018;10:28-31.
- Wong M, Lee J, Choy B, et al. Systematic Review and Meta-analysis on the Efficacy of Selective Laser Trabeculoplasty in Open-angle Glaucoma. Surv Ophthalmol 2015;60:36-50.
- Abuswider SA, Damji KF, Ritch R. Selective laser trabeculoplasty. In: Shaarawy TM, et al. eds. Glaucoma, 2nd ed. Elsevier; 2015:699-707.
- Khawaja AP, Campbell JH, Kirby N, et al. Real-world Outcomes of Selective Laser Trabeculoplasty in the United Kingdom. Ophthalmology 2020;127:748-57.
- Shazly TA, Latina MA, Dagianis JJ, Chitturi S. Effect of Central Corneal Thickness on the Long-term Outcome of Selective Laser Trabeculoplasty as Primary Treatment for Ocular Hypertension and Primary Open-angle Glaucoma. Cornea 2012;31:883-6.
- Garg A, Vickerstaff V, Nathwani N, et al. Primary Selective Laser Trabeculoplasty for Open-angle Glaucoma and Ocular Hypertension. Ophthalmology 2019;126:1238-48.
- Hutnik C, Crichton A, Ford B, et al. Selective Laser Trabeculoplasty versus Argon Laser Trabeculoplasty in Glaucoma Patients Treated Previously with 360° Selective Laser Trabeculoplasty. Ophthalmology 2019;126:223-32.
- Barkana Y, Belkin M. Selective Laser Trabeculoplasty. Surv Ophthalmol 2007;52:634-54.
- Koucheki B, Hashemi H. Selective Laser Trabeculoplasty in the Treatment of Open-angle Glaucoma. J Glaucoma 2012;21:65-70.
- Benetz BA, Lass JH. Specular Microscopy. Cornea 2018;37:7-8.
- Hillenaar T, Cleynenbreugel H, Remeijer L. How Normal Is the Transparent Cornea? Effects of Aging on Corneal Morphology. Ophthalmology 2012;119:241-8.
- Ong K, Ong L, Ong LB. Corneal Endothelial Abnormalities After Selective Laser Trabeculoplasty (SLT). J Glaucoma 2015;24:286-90.
- Liu ET, Seery LS, Arosemena A, et al. Corneal Edema and Keratitis Following Selective Laser Trabeculoplasty. Am J Ophthalmol Case Rep 2017;6:48-51.
- Regina M, Bunya VY, Orlin SE, Ansari H. Corneal Edema and Haze After Selective Laser Trabeculoplasty. J Glaucoma 2011;20:327-9.
- Srinivas SP. Dynamic Regulation of Barrier Integrity of the Corneal Endothelium. Optom Vis Sci 2010;87:239-54.
- Patel SB, Pasquale LR. Laser trabeculoplasty. In: Spaeth GL, et al. eds. Ophthalmic Surgery: Principles and Practice, 4th ed. Elsevier; 2012:302-7.
RELATED VIDEOS
To learn more about the YC-200 S plus YAG/SLT, visit: https://usa.nidek.com/yc-200/
To learn more about the CEM-530 Specular Microscope, visit: https://usa.nidek.com/cem-530/